
National Institute of Allergy and Infectious Diseases, NIH
How did coronavirus spread across the world? Why is it so bad?
And other coronavirus questions, answered by an epidemiologist

Epidemiology
Ed: Even though we've been reading one article after another about SARS-CoV-2, the novel coronavirus, some basic facts about the crisis were still unclear to us. How did this all begin? Why is this virus so problematic? How is it spreading? We asked epidemiologist Beth Linas to answer these questions, and more.
The virus apparently emerged in Wuhan, China. How does a virus that starts in one place spread around the world?
The short answer is that we live in a global economy that includes frequent domestic and international travel, and viruses often hitch rides with us.
Viruses, like other pathogens, don't produce symptoms as soon as they come into contact with humans. First, they go through an incubation period, or a period of time when the virus multiplies to a threshold necessary to produce symptoms in its host. During the incubation period, your body's immune system recognizes the virus, and reacts through multiple kinds of immune responses. If your immune system can keep the virus population in your body below the threshold, you won't experience symptoms (but may be able to still spread some viruses). The effectiveness of an individual's immune system in responding to the virus also plays a role – some people can stave off viruses longer than others.
For clarity, SARS-CoV-2 is the virus responsible for the novel coronavirus disease. The World Health Organization’s (WHO) chosen name, COVID-19, is just short for "coronavirus disease 2019" and their preferred nomenclature for the virus is "the virus responsible for COVID-19" or "the COVID-19 virus."
This incubation period between infection and symptoms allows pathogens to move stealthily across borders before being detected. It is likely that travelers passing through Wuhan were unknowingly encountering people who were infected with SARS-COV-2, the virus that causes the disease known as COVID-19. These travelers may have returned home without knowing they were infected.
The incubation period of COVID-19 virus partially explains how the disease spread so widely before being detected. The WHO currently estimates the incubation period for COVID-19 to range from one to 14 days, most commonly around five days (for comparison's sake, the flu's incubation period is about two days). However, these estimates could change as we get a better understanding of the disease. Such a long incubation period, combined with the possibility that people can possibly spread the disease without showing symptoms, would also help explain its spread.
Light refraction shows change in air density after coughing.
Gary S Settles, Penn State University, via NIH
Other specific features of SARS-CoV-2 can also help explain how it is making its way around the world, particularly how it moves between people and its infectiousness.
We know that SARS-CoV-2 is spread through person-to-person contact. Specifically, the virus spreads through droplets that form when an infected person coughs or exhales. Sneezing is not a common symptom of COVID19. Those droplets land in the mouths or noses of people who are in close contact (within 6 feet, according to the CDC).
It may also be possible for individuals to become infected with COVID-19 by touching surfaces or objects that has the virus on them (a surface carrying a potential infection is called a "fomite") and then touching their own eyes, nose, and mouth. A study by scientists at the US National Institute for Allergies and Infections Disease, posted as a pre-print on medRxiv, includes findings that SARS-CoV-2 can persist for up to three days on plastic and steel surfaces.
Airborne transmission has not been reported for COVID-19, and it is not believed to be a major mode of transmission based on available evidence. Typically, airborne transmission describes particles that can suspended in air. Measles and tuberculosis (TB) are examples of airborne pathogens. Tiny aerosols can potentially stay in the air for longer and travel further than comparatively large respiratory droplets. The distinction between whether a pathogen can become airborne is thought to depend on its size, however, this delineation is not clear cut.
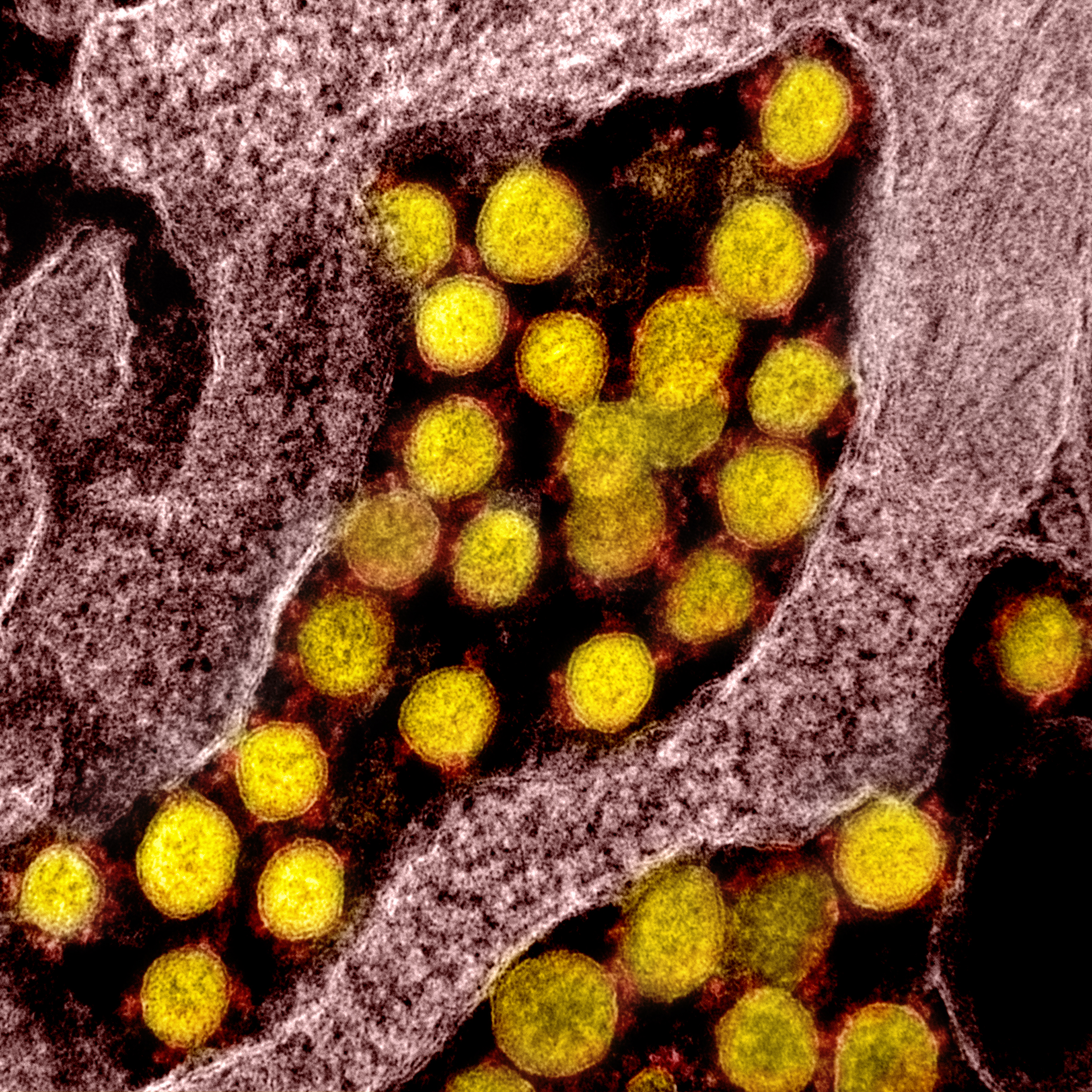
Coronavirus (SARS-CoV-2, in yellow) particles isolated from a patient
National Institute of Allergy and Infectious Diseases, NIH
To further understand virus spread, epidemiologists examine its serial interval, or the duration of time between the onset of symptoms between cases. The serial interval helps identify how cases are related to each other (who infected whom), and can aid in determining appropriate procedures for infection control.
One study in Japan, published in early March, approximated the serial interval for COVID-19 to be about four days, which is shorter than its incubation period. Because COVID-19's serial interval is shorter than its incubation period, many people are likely spreading it before they even show symptoms.
Another feature of infectious diseases that is often cited when examining spread is the basic reproductive number, R0 (pronounced "R-naught"), or the average number of people who will become sick from a single infected person in a population who have never encountered the disease before. If R0 is less than 1, each infection leads to less than one new infection. In this case, the disease will eventually die out. If R0 is greater than 1, each existing infection leads to more than one new infection. The disease will spread between people, and may lead to an outbreak or epidemic.
R0 is used as an indicator of the contagiousness or transmissibility of infectious agents. Early estimates from Wuhan put COVID-19's R0 at 2.2. This means that, on average, one new case is expected to infect between two and three people in an entirely susceptible population. The R0 for COVID-19 is larger than H1N1 (swine flu), which had an R0 of 1.4-1.6, and is roughly comparable to Ebola (R0 of 1.5-2.5) and SARS (R0 of 2-4). It's much lower than smallpox (R0 of approximately 6.9), and measles (R0 of 12-18, but with substantial variation). These values tell us COVID-19 is more infectious and easily transmitted than the swine flu, which caused a pandemic in 2009, but less infectious than smallpox and measles.
Why is there a gap between when a virus (apparently) arrives in a community and when visible cases start to emerge?
This comes back to the incubation period – it can take two weeks for person to show symptoms after coming into contact with the SARS-CoV-2 virus.
For comparison, the incubation period for measles averages about 10-14 days, but ranges from 7–23 days. The incubation period for SARS is 3-5 days with a range of 2-7 days.
Is it possible to know why COVID-19 is spreading so much farther than related viruses like SARS and MERS did?
This is still under investigation, with new data available every day. Beyond features of virus spread, sometimes it is helpful to look at other aspects of a virus to better understand how it behaves.
The case fatality rate (CFR), which is the number of deaths from a given disease divided by the total number of people with confirmed illness, can be used as a measure of disease severity. The global fatality rate for COVID-19 was initially reported as at about 2.3%, though WHO reporting has increased this rate to 3.4%.
SARS and MERS have higher case fatality rates than COVID-19. The 2003 outbreak of SARS had a case fatality rate of around 10% (774 deaths out of 8098 cases), while MERS has killed 34% of people with the illness between 2012 and 2019 (858 deaths from 2494 cases). However, COVID-19 has lead to more total deaths because more people have been infected.
One hypothesis for the higher case fatality rates with SARS and MERS compared to COVID-19 is related to secondary infections (infections that occur during or after the initial infection). Most secondary infections from SARS and MERS occurred in hospitals, which prevented community spread of the virus. With COVID-19, we may be seeing more secondary infections and subsequent community spread as a result of primary cases not being tested, either due to lack of tests or lack of severe symptoms.
This community spread will continue as we are still having difficulties in identifying and counting mild cases of COVID-19. It currently seems COVID-19 is just as transmissible as SARS and MERS but not as deadly. However, everything we know about the virus, including R0 and case fatality rates, is preliminary and will evolve as the pandemic does.
The World Health Organization has officially declared this outbreak a pandemic and the public health community is continuing to work diligently to further our understanding of this novel disease and to prevent it from spreading. As such, we now must use one of our more stringent methods to slow the spread of this infectious disease and this includes limiting all unnecessary movement and gatherings, including working from home if possible, limiting unnecessary travel, and avoiding large crowds like those at concerts or sporting events.
It is time to approach our daily lives differently. While everyone can't enact all social distancing measures, individual actions make a big difference. As always: please continue to wash your hands, refrain from touching your face, and stay home if possible. Being prepared is a great way to reduce anxiety and panic.
.jpeg?auto=compress%2Cformat&crop=faces&fit=crop&fm=jpg&h=800&q=70&w=1200)
















